
SGECR Occasional Series No.1

Mixed Blessing: The Impact of Suttonian Smallpox Inoculation in the later Eighteenth Century
Robert Dimsdale (St.Aubin-Sauges, Neuchâtel)
Introduction
At the outset of the eighteenth century, many peoples world-wide had long exercised preventive measures to procure a degree of protection against epidemic smallpox, this being as true for Europeans as for others. By the early 1720s one such measure, which originated in Greece, had been imported from the Ottoman Empire to Britain and by mid-century it had become widely known in Europe and North America as inoculation. The operation was called inoculation in both French and English and it was only much later that the term variolation was coined in order to distinguish it from other kinds of inoculation which were nothing to do with smallpox, but for the purposes of this study the term inoculation as used in all the eighteenth-century historical sources is retained [1].
It was not, however, widely used, although there was increased inoculation in the 1750s, but by the 1760s a particular version known by the name of its inventor as Suttonian inoculation met abruptly with such success locally in England that by the century’s close it was spreading throughout Europe and beyond to much of the rest of the world. The practice was flawed, since as well as protecting the inoculated it could also spread smallpox to the uninfected, and at the very close of the century it was suddenly superseded almost universally by another practice, known as vaccination, which was not subject to this flaw. This account is a consideration of the inception, progress and influence of Suttonian inoculation in the course of the second half of the eighteenth century. Its principal sources are the publications of that period and recent historical interpretations. Its appearance in the Newsletter of the Study Group on eighteenth-century Russia is attributable to the signal personal intervention of Empress Catherine II in 1768 and the essay’s aim is to put that intervention into perspective. It is sustained by the belief that the period is deserving of further consideration on its own account and not just as a rehearsal for the arrival on the scene in 1798 of Edward Jenner’s published description of vaccination.
‘Les maladies contagieuses telles que: petite vérole, rougeole, scarlatine, peste, choléra etc. sont considérées par les Géorgiens comme des esprits munis de la substance humaine, un peu plus délicate, il est vrai, avec les manifestations et des faiblesses analogues à celles de tous les mortels.’ [2]
In these terms Tedo Sakhokia commenced his description of the cult of smallpox in Georgia in a paper published by the Anthropological Society of Paris in 1903. He described how the Mingrelians coped with their natural terror when repeatedly confronted with deadly epidemic diseases. Mingrelia is the westernmost province of Georgia and has a Black Sea coastline, at times visited by Turkish sailors bringing smallpox with them. The afflicted inhabitants associated the disease with lordly spirits both good and bad called ‘Batonébis’, who arrived in their dreams and who had to be appeased and placated at all costs. [3] Like the infection, the spirits wafted in effortlessly. The well-disposed ones were beautiful women clad in white and riding white mules, and the inimical – some Christian, some Muslim – rode black ones. All manifestations of the disease had to be cherished so as not to displease them, for they would – if not humoured at every turn − round on the sick and kill them. Any disrespect of smallpox symptoms was sure to provoke their wrath and vengeance, for the symptoms were themselves the ‘Batonébis’. The rules for pandering to their many whims covered all aspects of what amounted to a comprehensive regime for patient care. How the sickroom had to be arranged and decorated: what the bedclothes should be made of and how managed: what the patient’s diet should be: the arrangements for medical supervision and visiting: and also for smoking, which was usually banned indoors: all were prescribed. Some of the supposed preferences of the ‘Batonébis’, such as a predilection for goats’ meat and blood, reflected those of the Mingrelians themselves. Others, such as the arrangements for quarantine, reflected responses which they had developed to face epidemics, particularly flight. All in all a coherent strategy couched in eminently practical terms but based on spiritual imperatives. Sakhokia was writing about the situation in the later nineteenth century. He reckoned that Jennerian vaccination had made little headway in Mingrelia at that time and that he was observing an ancient example of a universal defence mechanism. [4]
Whether Sakhokia’s account can be corroborated or not, it is certain that – sometimes apparently in isolation – many peoples [5] adopted a strategy to combat the terrifying onset of smallpox which was of considerably more practical use than the house-keeping developed by the Mingrelians, and which can be described as folk inoculation. Why they did so is clear enough. They were driven by fear. How they developed it is a process best explained by anthropologists and ethnologists. Versions of it cropped up in nearly every part of the world. Prominent in all coverage of this phenomenon [6] are parts of China – very early in the field − and parts of the Indian sub-continent (perhaps even earlier), parts of Africa and Asia, the Ottoman Empire and Europe. Reduced to essentials folk inoculation consisted of inserting smallpox pus or other smallpox-infected matter into a healthy subject or applying it in some way to the skin thereby inciting a mild form of the disease and mysteriously – and still today imperfectly understood − conferring immunity from the dangerous natural smallpox. Similarly extensive was the practice of exposing children to mild cases.
The custom had taken hold in widely separated localities and maintained itself within them without it becoming ubiquitous. Was this because unsophisticated and static peoples or discrete ethnic groups were constrained by geographical location or otherwise disinclined to proselytise? Was there sometimes an element of emulation brought about by rumour, trade or other interaction with a wider world? Had it once been a universal and innate human response, which only faded with population growth and changing settlement patterns? Or yet again might the erratic and limited spatial distribution of folk inoculation have been a consequence of fitful patterns of epidemics and the waxing and waning of the potency of Variola major [7] over time? Certainly a few peoples succeeded in generalising it to a significant extent, most importantly in south China and large areas of India [8] .
Be it as it may, what induced a step change for Europe was the occurrence of the folk practice in a major port city, to which it had been introduced. The city was Constantinople, capital of the Ottoman Empire and a focus for many peoples. The folk practice which began to operate there came from the Peloponnese [9] , and it was this version which was described by literate observers and medical operators and transferred into the stream of such relevant literature as there was in a few western European centres. Furthermore it stepped straight into a fast lane by being transmitted to a court circle from which radiated channels of communication which could and did propagate the idea and the practice. From the start the culture of the new host made alterations to the folk procedures and adapted them to that host’s prevailing medical practices and notions.
Western absorption of inoculation earlier in the eighteenth century was, however, small scale and spasmodic. Until the 1750s – with a few exceptions – inoculation was restricted to people willing to take the risk and able to bear the cost, but then – driven by major epidemics – there was a geographically uneven surge culminating in what can fairly be termed a paroxysm in the late 1760s, the effects of which fitfully widened and deepened acceptance up to the end of the century and beyond. This acceptance fused with much of the rest of the world through the European-based empires, where it encountered the pre-existing traditions of folk inoculation and attempted to supplant them.
At the eighteenth century’s end a new technique – vaccination described by Edward Jenner (1749-1823) [10] – emerged and very quickly started along the path which was being so erratically and fortuitously beaten by inoculation, so that 180 years later it succeeded in eliminating smallpox. Once again the disease was mastered in the West before it was overcome in many other parts of the world. Even in the eighteenth century there were sparks of understanding that smallpox could be eliminated, but in the nineteenth and twentieth centuries these sparks became a slow-burning fire, which was only belatedly fanned into an all-consuming conflagration under the auspices of the World Health Organisation [11] .
So much for ‘la longue durée’ and the setting for a description of the crucial role of a new kind of inoculation in the second half of the eighteenth century – a method which over little more than thirty years from 1768 was employed, albeit unevenly, to transform humankind’s defence against smallpox. What came to be widely known as the Suttonian system was developed and refined by the Englishman Robert Sutton (c.1707-1788) − a Suffolk surgeon. In its essence his method depended upon the slightest of incisions, fresh smallpox matter and the cold method. [12] All these elements ran counter to what had previously been common practice, typically including the making of major incisions enclosing lint imbued with smallpox matter in various types and states, and keeping patients warm. Sutton sought a relatively simple and straightforward system in the expectation that it would engender mild symptoms (few pocks) and thereby reduce the risk to the patient. He worked on the development of his method between 1755 and 1763, by which date he had perfected it. He may have been motivated to improve inoculation by an unfortunate experience − his eldest son had contracted a bad case of smallpox following inoculation by a neighbour. Through experiment he satisfied himself that he could usually attenuate the symptoms and conduct patients through the inoculated complaint with relative impunity. [13] Aspects of his method drew on those of precursors but his merit lay in the development over a number of years of an identifiable and successful system – one which was capable of being packaged and diffused. Robert himself left no description, but from evidence and interpretation supplied by his family and capable emulators it was roughly in accord with contemporary English medical notions and discourse. [14]
Not so was the technique of the Italian Angelo Gatti (1724-1798) Sutton’s gifted and university-trained mainland European contemporary, who also sought to attenuate the symptoms of inoculated smallpox [15] . Whereas Suttonian inoculation retained much of traditional preparation, Gatti confidently detected the readiness of a patient for inoculation by suppleness of skin and sweetness of breath, in most cases dispensing with preparation entirely, which in a few led to serious consequences. He was a distinguished operator on patients at the upper end of the social register where a mishap could easily bring inoculation into disrepute. Suttonian inoculation was not risk free, but in practice a death attributed to inoculation practiced on a large scale appeared as a proportionately insignificant blemish on what was broadcast as massive numerical success.
It seems clear enough that Suttonian inoculation even for a healthy patient was not risk free. At one end of the scale the operation might result in no pocks at all and at the other the pocks might verge on confluence, that is being so numerous as to be life threatening. One operator [16] recorded that over half his 188 patients exhibited less than thirty pocks whereas 20% had more than 100, with a few over 500 and one having 1,000. Large numbers of pocks on a patient were more likely to spread the disease to a nearby person who had never had the natural smallpox, but such infection could even be transmitted by someone showing no pocks whatever.
Knowledge of Suttonian inoculation remained local until one of Robert’s sons – Daniel Sutton (1735-1819) – realised that his father’s procedure was so simple and effective that it could be undergone by thousands of patients rather than tens, and set up and advertised an inoculation establishment to cope with very large numbers at Ingatestone, Essex, on a main road to and from London. At first it faced suspicion and fear that it would spread the disease, both on the part of the public and also the authorities of market towns – fearful of curtailment of markets and trade – but in in the spring of 1764 Daniel achieved a crucial breakthrough and – energetically promoted and organised – his system began to spread, at first to other parts of Essex and nearby Kent. [17] From the beginning Suttonian inoculation entailed a degree of preparation prior to inoculation, in common with the greatest part of the practice which preceded it, but with the difference and added cachet that it boasted a secret medicine, which was supposed to ensure success, and which made it the more attractive and marketable. Daniel Sutton was an exceptionally capable organiser and not only ran a highly effective in-house surgery and major inoculations in other areas but also set up franchises in order to profit from a wider and indeed international system of his brand of inoculation, which engaged several of his brothers and relations by marriage, as well as outsiders ready to participate in such a thriving and lucrative trade.
The Suttons had their own publicist the better to impress upon the market the advantages of their new inoculation, [18] but they needed to engage from the outset in a polemic against the competition which had already sprung up, typified most effectively by Thomas Dimsdale (1712-1800) from the neighbouring County of Hertfordshire who organised inoculations along Suttonian lines: created an up-market clinic at Hertford – the County town – and also published a convincing practical handbook on the new inoculation including case studies and designed to accommodate the system more explicitly to the prevailing medical scene and thought processes. [19]
The potential of Daniel Sutton’s breakthrough in Essex was therefore recognised locally, but also in London and in many European capital cities, courts and medical centres. Most of them were cognizant of the pre-Suttonian practice, which – particularly from the mid 1750s but in some cases from a decade earlier – had been exploited with some success, albeit on a limited scale. Théodore Tronchin (1709-1781) had provided a spark for inoculation campaigns – first in Amsterdam in 1748, where Thomas Schwenke and David Gaub were inoculating by 1754 and 1755 − and soon after in Geneva, his own home town. And the operation was being performed at the same time and by different people in Denmark, Norway, Sweden, Geneva, Italy, Livonia and St. Petersburg [20] [21] . But there were also setbacks. In France these mixed results had resulted in a prolonged public investigation [22] which involved the collection of evidence, among the best of which – from a Scottish source [23] – pointed to widespread inoculation in Scotland by surgeons and physicians not dependent on the Suttonian version. The French investigation was triggered by a well-publicised failure attributed to an inoculation case which had gone wrong. [24] As we have seen, the inoculator – Gatti – had developed a method at once simpler, more revolutionary and ahead of its time than that of the Suttons. It is not unlikely that Gatti and Robert Sutton were aware of one another’s aims and achievements [25] – at least their aims were the same and their techniques emerged at the same moment.
The French investigation showed sharply divided opinion in the medical profession, and inoculation was not comprehensively vindicated. It was deemed permissible, but not in towns [26] , and this approach and ruling was followed elsewhere in the West [27] .
Not so, however, in England, where Suttonian inoculation – in its essence if not its details – recommended itself to the most influential medical, court and diplomatic circles, which in turn recommended it to some of their peers elsewhere in Europe. At the centre of this development was John Pringle (1707-1782), an influential Scot who had made his name in military medicine. Pringle’s judgement had become the most respected at Court where he had the ear and the confidence of the King (George III, 1738-1820). News of Suttonian inoculation and its dramatic successes had also struck well-placed medically influential centres on mainland Europe with considerable force. Two of these − Vienna and St. Petersburg – determined independently of one another to implement the practice at much the same time. Vienna was first in the field, driven by Empress Maria Theresa (1717-1780), whose family had suffered grievously from smallpox. Her ambassador in London sought advice on who would be a suitable person to introduce the practice. To respond to the request and with the knowledge and support of the King, an ‘ad hoc’ committee was tasked with considering it [28] , but it was Pringle’s role which was decisive. He had himself interviewed Daniel Sutton and questioned him closely on his technique and methods. He was not entirely convinced of them in all details, but of the spectacular results he was in no doubt [29] . He also knew and was impressed by the abilities of a young doctor from the Austrian Netherlands – Jan Ingen Housz (1730-1799) [30] – and recommended him as the best person to carry Suttonian inoculation to Vienna. [31] Very early in 1768 Ingen Housz had assisted Dimsdale with a successful emergency inoculation of two villages in Hertfordshire [32] and Pringle had received detailed accounts of it from his protégé. Pringle was also aware of Dimsdale’s recent publication of an account of inoculation, which served as an endorsement of Suttonian inoculation. Very soon afterwards St. Petersburg, with the enthusiastic support – indeed leadership – of Empress Catherine II (1729-96) approached London in search of a suitable person to introduce Suttonian inoculation. In this case the Suttons themselves put in a bid [33] , but an offer was made to Dimsdale instead on the advice of a man who may have been the ambassador’s own physician, the Quaker John Fothergill (1712-1780) [34] . In this way the new technique jumped to pre-eminence in two major policy-making centres and was put to use by medical administrations there with varying success, superseding prior techniques and boosting inoculation. British policy on the matter, with reserved and cautious royal support, was to use the introduction of the technique as a friendly and disinterested gesture to take its place among more important diplomatic objectives. The King wished for a favourable outcome for Maria Theresa and her stricken family [35] and although he professed nervousness that a failure in St. Petersburg might jeopardise relations with Russia, he was supportive of that enterprise too [36] .
The rapid spread of Suttonian inoculation was effected by other means and on a broader front than the diplomatic, important and spectacular though that was. In 1768 more publications on inoculation, of which over half dealt with or referred to or were connected with the Suttonian technique were published in the West than in any other year in the eighteenth century.
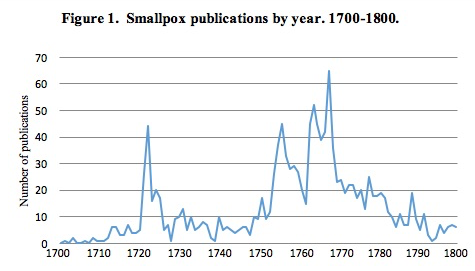
Figure 1 is a graph showing the number of publications on smallpox in every year of the eighteenth century, compiled principally from two contemporary German lists - by J. G. Krünitz [37] (1728-96) and F. Olberg [38] (1767-1840). There are at least 1,400 of these. This said, it should not be overlooked that this output of titles was dwarfed by the other manifestations of print and they were only a restricted part of the barrage of printed matter related to inoculation. For the century as a whole, the principal features are the introduction of inoculation in 1721-5 in English from England and New England: a serious engagement with it - most significantly in French, but also in German for a decade from the mid-1750s: a major output in 1767-8, with most titles in English, French and German but with significant numbers in Italian and Dutch, and in the 1770s − particularly towards the end of the decade − in English concerning how best to carry out the operation in London and larger towns, but also more generally in German.

More pieces were published in Latin than in any other language, mostly associated with Universities, and Figure 2 illustrates this continuous relatively low-level presence.

Figure 3 shows German language pieces - the next highest number - and appears to be a factor of the multiplicity of German states and universities, many keeping abreast of developments in the field at home and abroad and translating foreign language pieces where deemed of interest.
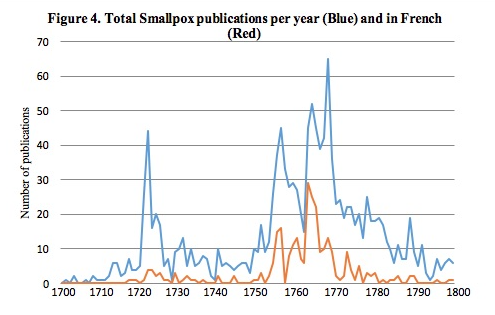
Figure 4 shows a striking concentration of publications in French for twelve years from 1755.

And Figure 5 shows the importance in English of the introduction of inoculation in 1721-5: the introduction of the Suttonian system in the late 1760s, and to a lesser extent the controversy over how to deal with smallpox in large towns in the late 1770s.
1768 is the year in which more was published on inoculation, and in more languages, than in any other single year in the eighteenth century, and the impact of the relative ease and simplicity of the Suttonian system, as well as the impetus afforded to it by Dimsdale’s publication and activities, are clearly apparent [39] . These titles are set out in Table 1. [40]
Table 1: 1768 Publications on Smallpox
| Country Place |
Author Suttonian Link |
Title |
|---|---|---|
| England | ||
| London | Gatti (A) | New observations on inoculation translated from the French by M. Maty |
| Dimsdale (T) | The Present Method of inoculating for the small-pox (4th edition) | |
| Percival (T) | On the disadvantages, which attend the inoculation of children in early infancy | |
| Ruston (T) | Essay on inoculation for the Small-pox … with an appendix containing a Chymical Examination of Mr Sutton’s medicines (2nd ed) | |
| Ruston (T) | Essay on inoculation for the Small-pox (3rd ed) | |
| Watson (W) | An account of a series of experiments instituted with a view of ascertaining the most successful method of inoculating the Small-pox | |
| Baylies (W) | Aphorisms on the Small Pox tending to investigate the true Nature of the Disease, whether acquired by contagion, or inoculation. And, to manifest the superior Rationality and Excellence, of the modern, over the antient Method of its Treatment | |
| Hallifax (J) | A sermon preached in the parish church of St Bride, London, on Thursday, April 28, 1768, Before the President, Vice-Presidents, and Governors of the hospitals for the small-pox and inoculation | |
| Anon | Raisons de l’inoculation de la petite vérole par lesquelles on fait voir que cette méthode n’est aucunement contraire à la religion & à la raison; mais un devoir qu’exigent l’une & l’autre | |
| Maty (M) | A Short Account of the Manner of Inoculating the Small Pox, on the Coast of Barbary, and at Bengal, in the East Indies, Extracted from a Memoir Written in Dutch, by the Reverend Mr. Chais, at the Hague | |
| Russell (P) | An Account of Inoculation in Arabia, in a letter from Dr. Patrick Russell, Physician at Aleppo, to Alexander Russell | |
| Anon | An Account of the Rise, Progress and State of the Hospitals for relieving poor People afflicted with the Small-Pox, and for Inoculation from its First Institution (26 September 1746) to 24 March 1768 | |
| Anon | Inoculation for the small pox manifested not to be repugnant to Religion or Reason but rather an incumbent duty in obedience to both | |
| Jones (H) | Inoculation; or Beauty’s Triumph: A Poem in two Cantos | |
| Scotland | ||
| Edinburgh | Silver (T) | … de variolarum insitione … |
| Ireland | ||
| Dublin | Houlton (R) | Indisputable facts relative to the Suttonian art of inoculation. With observations on its discovery, progress, encouragement, opposition, &c. &c. |
| Gatti (A) | New observations on inoculation (tr. M. Maty) | |
| Watson (W) | An account of a series of experiments instituted with a View of ascertaining the most successful Method of inoculating the small-pox | |
| Percival (T) | Arguments against the inoculation of children in early infancy | |
| Closs (J. F.) | A New Method of curing the small-pox; By which that Disease, taken in the Natural Way, is rendered as Void of Danger as when Received from Inoculation with a Specimen of Miscellaneous Observations on medical subjects (tr. from the Latin) | |
| Holland | ||
| The Hague | Chais (C) | Lettre à Sutherland, associé de Sutton, sur la nouvelle méthode d’inoculer la petite vérole, et réponse du Dr. Sutherland |
| Chais (C) | Brief aan den heere Sutherland over de nieuwe wyze om de Kinderpokjes in te enten | |
| Wilkes (J) | Suttonius, ou le Magicien Blanc, nouvelle nouvelle | |
| Amsterdam | Ingenhousz (J) | Lettre de Monsieur Ingenhousz, Docteur en Médecine à M Chais … au sujet d’une Brochure, contenant sa Lettre à Mr. Sutherland, & une Réponse de Mr Sutherland à Mr. Chais, sur la nouvelle méthode d’inoculer la petite vérole |
| Anon | Onderzoek, Of men zich door de Suttonianen, dan volgens de manier van Dimsdale, moet laaten inënten in een Brief Strekkende tot Antwoord op een Brief van een’ Vriend uit den Haag, aan zynen Vriend te Rotterdam | |
| Watson (W) | An account of a series of experiments instituted with a view of ascertaining the most successful method of inoculating the Small-pox (Dutch tr.) | |
| Gatti, A | Nouvelles Réflexions sur la Pratique de l’Inoculation | |
| ‘s-Gravenhage | Sandifort (E) | Verhandeling over de tegenwoordige manier van Inenting der Kinder-pokjes … door Thomas Dimsdale, M.D. uit het Engelsk vertaald … |
| Anon | Oordeel van de genees- en heelmesters van den Koning van Engeland, aangaande de manier van inentinge der kinder-pokjes der Heeren Suttoniaanen | |
| Van Rosenstein | Handleiding tot de Kennis Van Geneezing Van de Ziekten Der Kinderen. ... In het Zweedsch geschreeven Door Den Heere Rosen Van Rosenstein | |
| Leiden | Evans (J) | De variis methodis inserendi variolas |
| Rotterdam | Anon | Brief van een Vriend uit den Haag aan zynen Vriend te Rotterdam Behelzende een onderzoek of men zich door de Suttonianen, dan volgens de manier van Dimsdale, moet laten Inënten |
| Belgium | ||
| Liège | Baylies (W) | Aphorismes sur la petite vérole |
| France | ||
| Paris & Nancy | G. de Foigny | Traité-pratique de l‘inoculation conduite relatives au choix de la saison propre à cette opération; de l’âge & de la constitution du sujet à inoculer; de la préparation qui lui convient; de l’espèce de méthode qui doit être préférée; & du traitement de la maladie communiquée par l’insertion |
| Paris | Paulet (J J) | Histoire de la petite vérole avec les moyens d’en préserver les enfans et d’en arrêter la contagion en France |
| Paulet (J J) | Mémoire pour servir de suite à l’histoire de la petite vérole … | |
| Power (J) | Lettre sur les Progrès de la nouvelle Méthode d’inoculer du sieur Sutton. (Journal de médecine, chirurgie et pharmacie) | |
| Dubourg (J B) | Opinion d’un médecin de la Faculté de Paris sur l’inoculation de la petite vérole | |
| Dubourg (J B) | Mémoire à consulter et consultation pour Me Jacques Barbeu du Bourg et consorts, tous docteurs régents de a faculté de médecine de Paris | |
| Gardane (J J de) | Mémoire dans lequel on prouve l’impossibilité d’anéantir la petite vérole pour faire suite aux observations sur la meilleure manière d’inoculer | |
| Condamine de la | Mémoires pour servir à l’histoire de l’inoculation de la petite vérole, lu à l’Académie des Sciences en 1754, 1758 et 1765 | |
| Anon (?Thurant) | Examen des principaux points de la réponse à l’argument tiré du nombre des personnes mortes en Angleterre de la petite vérole | |
| Anon (?Thurant) | Mémoire sur le fait de l’inoculation | |
| Taconet | La Bourbonnaise inoculée | |
| Lyon | Gontard (J A) | Du traitement et de l’extinction de la variole et de la rougeole |
| Barthenheim | Hertzog (F A) | De emolumentis in genus humanum ex variolarum insitione fluentibus |
| Switzerland | ||
| Zürich | Schinz, (S) | Neue Methode für die Einpfropfung der Pocken welcher als ein Anhang beygefüget sind einige Versuche über den Erfolg einer ähnlichen Verfahrungsart bey den natürlichen Pocken von Thomas Dimsdale, M.D. aus dem Englischen nebst einigen dieser Uebersetzung beygefügten |
| Winterthur | Anon | Inokulations Geschichte von Winterthur |
| Germany | ||
| Berlin | Königsdörfer (G) | Memorial an alle, die die Kinderblattern noch nicht gehabt haben |
| Breslau | Morgenbesser(J) | Gedanken von der Nothwendigkeit der Zubereitung von der Einpfropfung der Kinderblattern |
| Frankfurt | Baylies (W) | Aphorisms on the Small Pox, Tending to investigate the true nature of the disease, whether acquired by contagion, or inoculation. And, To manifest the superior rationality and excellence, of the modern, over the antient method of its treatment. |
| Gotha & Göttingen | Von Schlözer (A L) | Von der Unschädlichkeit der Pocken in Russland und von Russlands Bevölkerung überhaupt |
| Grünstadt | Wolf (J H K) | Die Pflicht, durch die Einpfropfung der künstlichen, den natürlichen Blattern zu entgehen |
| Hamburg | Anon | Unterthänigstes Memorial des herrn D. zu Altenburg Königsdörfer und eines andern deutschen Arztes an alle, die die Kinderblattern noch nicht gehabt haben |
| Langensalza | Baldinger (E) et al | Der Herrn Tissot und Rosenstein Abhandlungen von der Natur und Kur der Kinderblattern zum nützlichen Gebrauch |
| Leipzig | Krünitz (J G) | Verzeichnis der vornehmsten Schriften von den Kinderpocken und deren Einpfropfung |
| Tiemann (C) | D. Thomas Dimsdales Unterricht von der gegenwärtigen Methode, die Kinderblattern Einzupfropfen … Aus dem Englischen übersetzt … | |
| Münich | Leuthner (J) | Auszug von der heutigen Inokulations-Geschichte in England des Herrn Thomas Dimsdale, der Arzneygelehrtheit Doctors in London … |
| Tübingen | Diez, Gmelin | De nova methodo inserendi variolas Anglicana |
| Hübner, Sigwart | De me ipso olim varioloso et morbilloso | |
| Unknown | Anon | Bewährung daß die Einpfropfung der Blattern nicht nur nicht wider die Religion und Vernunft ist, sondern vielmehr dem Gehorsam gegen beide zur Pflicht oblieget |
| Austria | ||
| Vienna | Locher (M) | Observationes practicae circa inoculationem variolarum in neo-natis institutam (Three publications) |
| Italy | ||
| Naples | Houlston (T) | Il presente metodo d’innestare il vajuolo Al quale sono aggiunti Alcuni sperimenti, istituiti colla mira di scoprire gli Effeti d’una somigliante condotta nel Vajuolo Naturale Del Dottor Tommaso Dimsdale, ... Tradotto in Italiano dalla terza edizione di Londra Con alcune Osservazioni, e Note ... |
| Padua | Caldani (L) | Innesto felice di vajuolo instituito e descritto |
| Venice | Vicentini (F) & Paitoni (G) | Prima memoria dell’ eccellente Dr Francesco Vicentini, intorno all’ utilita dell’innesto del vajuolo. Seconda memoria dell’ eccellente Dr Francesco Vicentini intorno alla scelta del miglior metodo d’innestare. Diario delle inoculazioni per commando dell’ eccellentissimo senato e del magistrato eccellentissimo della Sanita’ eseguita dall’eccellente Dr Francesco Vicentini medico fisico con la sopra intendenza dell’eccellente Dr Gio. Battista Paitoni protomedico. Relazione dell’ inoculazione del vajuolo ese[g]uita in Venezia nel Novembre del 1768 per decreto dell’ Eccelentissimo Senato descritta e presentata All’ Eccellentissimo Magistrato alla Sanita’ di Venezia da Giovambatista Paitoni |
| Zulatti (A) | Notizie degl’ innesti di vajuolo fatti in Cefalonia | |
| Unknown | Gatti (A) | Nouvelles réflexions (tr. into Italian) |
| Russia | ||
| St Petersburg | Jänisch (J) | Kurze Geschichte und Beschreibung der vorteilhaftesten Art, die Pocken einzuimpfen |
| Bakherakht (A) | Opisanie i nastavlenie o privivanii ospy | |
| Moscow | Zybelin (S) | Slovo o pol’ze privivanii ospy i preimushchestve onoi pered estestvennoiu, s moral’nymi i fizicheskimi vozrazheniiami protiv nepravomysliashchikh, govoren 5 dekabria 1768 g. |
| Neve (C de) | Diss. De variolis |
Sources: Krünitz, Verzeichnis der vornehmsten Schriften von den Kinderpocken und deren Einpfropfung, (Leipzig, 1768); F. Olberg, Beiträge zur Litteratur der Blattern und deren Einimpfung, vom Jahre 1768 bis 1790 (Halle, 1791); A.C. Klebs, Bibliography of variolation (Yale, 1913), and internet search.
The titles for 1768 identified to date number 73, of which 48 relating to Robert Sutton’s procedure (author’s name underlined) appeared in seven languages − fifteen in English, ten in French, nine in German, six in Dutch, three each in Italian and Latin and two in Russian. The influence of Suttonian inoculation may be understated as it has not been possible to inspect all the titles, and in addition authors such as Paulet and Gontard who advocated different approaches could not have been unaware of it. Some titles were published in one country and language about another, for example Von Schlözer’s German language piece about Russia, and others in translations, for instance Maty from Gatti’s French in London and Tiemann and Leuthner from Dimsdale’s English in Leipzig and Munich, but most vernacular titles are in the language of the place where they were published. And nearly all were private initiatives by authors, translators and publishers.
The 1768 list fits some known trends in the spread of information and the development of publishing in the second half of the eighteenth century. Medicine, mathematics and science as a category rose as a proportion of the total output of English-language books from 1763 to 1783 reflecting an increasing output of monographs, such as books on inoculation, rather than periodicals, which only claimed an increasing share of the market towards the close of the century. Latin still clung to its role as a ‘lingua franca’ and was indeed in evidence, but apart from its use for all the theses, was only present in terms of the inoculation debate in the publications of Maximilian Locher at Vienna. The replacement of Latin by the vernacular might suggest that knowledge was being directed into or emerging in unconnected linguistic pools, but this was not so, for translation was stepping in to reinforce communication between them, and in the case of several of the books on inoculation − notably Schinz’s Zürich German language version [42] of Dimsdale, for whose writing he nevertheless professed profound admiration − the translation was augmented by the translator’s sometimes decided contrary views, based on his own experience. And books on inoculation, while primarily of interest to professionals, were early contributors to the vogue for vulgarisation because the operation was often performed by all manner of unqualified people. Another trend illustrated by the translations from English into other languages is that of a growing interest in English ideas, sometimes characterised as ‘Anglomania’, although this is only one feature of the nascent contribution in the later eighteenth century of the vernacular − allied to print capitalism − to the growth of nationalism [43] .
This flood tide of essentially practical titles was identified and analysed by the distinguished Swiss physician Arnold Klebs (1870-1943) much of whose career was spent in the United States, where he rose to prominence in the campaign against tuberculosis. He retired to Switzerland in 1910: made a collection of eighteenth-century inoculation titles, which he bequeathed to Yale University [44] , and published two overlapping articles – one in English [45] and the other in German [46] – constituting an analysis of inoculation in the West. As a physician and researcher himself he had a sharp eye for the most impressive operators, such as the Genevan Théodore Tronchin (1709-81): innovators, such as Gatti, and physicians who were most effective as writers, such as the Vaudois (Swiss) Samuel-Auguste Tissot 1729-97), and he was at pains to account for the advances and setbacks of inoculation throughout the West by familiarising himself with the contents of his collection of titles through a network of correspondents and translators. Klebs concluded that inoculation was slowly gaining ground and that until the advent of Jennerian vaccination at the close of the century it bid fair to establish itself as the remedy of choice [47] . Since he wrote, much work on what occurred in many countries and languages has been published, shedding more light on and generally in support his conclusions. What follows here is not an exercise intended to catalogue the experience of inoculation country by country and empire by empire but an attempt to highlight those issues and personalities which and who loomed largest to contemporaries and, through them, trace the influence and impact of Suttonian inoculation during and after its initial launch.
The Franche Comté is a former Habsburg possession incorporated into France in the course of the state’s drive to establish a frontier to the south-east on the Jura range. In Besançon in 1765, just when inoculation was beginning to make some impact, a death resulted – apparently from inoculation [48] . The most successful inoculators would feature compelling statistics designed to show the impressive number of successful inoculations by reference to an insignificant number of deaths which had occurred. The ratio was a measure of success. There were also well publicised failures which were attributed to some or other mistake which had been made, or to some unusual circumstance, and supporters of inoculation turned such events into arguments in support of their case. The deaths must very often have been the consequence of some pre-existing ill health or weakness which gave rise to a fatal outcome, or at least aggravated an inoculation which had given rise to unusually serious symptoms, such as very large numbers of pocks. However a feature of pre-Suttonian inoculation was that deaths following inoculation – often of prominent patients – would be given local publicity and would stem inoculation initiatives in an area sometimes for years. In the Besançon case – very unusually – it had the opposite effect. A provincial physician, Jean-François-Xavier Girod (1735-83), had been recognised by the relevant medical official as being an excellent candidate for the post bearing responsibility for dealing with epidemics in the Province [49] , and it was Dr. Girod who was so challenged by the setback, but also so convinced by the potential and worth of inoculation, that he set to work to generalise it so as to afford protection against smallpox to as many of the inhabitants as he could. He was impressed by inoculation as carried out in England at the time and travelled there on two occasions − the second being to ascertain whether there was any truth in a criticism that the system as practiced there was causing fatalities [50] . He concluded that there was not, and succeeded over several years, by means of inspiring trust in the population and by organising a sufficient number of dedicated operators, in coming as close as anyone at that time to comprehensive coverage. The State chipped in with annual grants for the campaign’s expenses and there was recognition for Girod at the highest level. Although he was himself averse to reward he accepted an order and an honorary appointment as a royal physician and was regarded with affection by the King. Closer to home he declined a substantial recompense offered him for inoculating members of the Chalon family, but accepted in lieu their feudal rights in local forests, which he transmitted to his home village, Mignovillard. And at his death he was eulogised in the forum of the nation’s foremost medical institution [51] . Girod’s successful career in inoculation at a local level was unmatched in European terms so neatly did his selfless onset dovetail with the apparatus of government, within which it flourished and was sustained. Its singularity was, however, something of an exception proving a rule. The reception of inoculation in France was never straightforward and the operation suffered repeated setbacks there up to the end of the century. Nevertheless the Franche Comté experience provides a demonstration of the elements – from base to apex – concerned with the reception and the implementation of inoculation – the head of state, the Court, the Ministry, the medical authority, and at de-centralised level the Governor, his medical advisers and administration, the rank and file doctors and operators, and the people themselves.
Another operator, the little known Thomas Houlston, (1745-1787), who was an English medical graduate from Leiden − not to be confused with Robert Houlton, the Suttons’ publicist − was remarkably influential in the introduction of the system to several parts of mainland Europe. He inoculated at Vienna and Linz in 1768, [52] coinciding with Ingen Housz, before moving on to the Veneto and Naples, where he arranged for the translation of Dimsdale’s ‘The Present Method …’ and the publication of an Italian edition, dedicated to Grand Duke Leopold of Tuscany, himself shortly to be inoculated by Ingen Housz, [53] which included some of Houlston’s own case notes.
In the summer of 1770 he moved to Montpellier, which was in the throes of a smallpox epidemic, and where − in spite of several prominent old-style inoculations − the operation had never caught on. There he met another young Englishman − Dr. Batt, shortly to gain his medical degree at the University − and with him conducted some inoculations locally. The subsequent campaign of Suttonian inoculation, which spread westward to Béziers, is described in Foucquet’s 1772 publication, which contained a translation of Dimsdale, but also included a review of the contemporary European inoculation literature demonstrating the extent to which it was it was dominated by Sutton as represented by Dimsdale, and also an account of how it was able to overcome the long sequence of local false starts which was such a feature of the old method. [54] In fact the exercise may have been yet another short-lived one as both Houlston and Batt appear to have left for home by 1773 and I do not know whether or to what extent the Montpellier campaign persisted, but Foucquet’s account remains a telling exposé of how the system took hold there.
As heads of state Empresses Catherine and Maria Theresa and Kings Frederick II (1712-1786) and George III acted within specific settings and adopted strategies calculated to support foreign policy objectives as well as domestic ones. Inoculation, although only ranking as a secondary issue, impinged on both the ever present international diplomatic merry-go-round and the domestic scene. And it recommended itself in various ways to these heads of state as a sphere of influence appropriate to their own personal opinions and circumstances. Catherine had felt humiliated and anguished at having to avoid the Court at St. Petersburg so as to place herself and her heir out of harm’s way when she knew that there was a remedy available which would obviate the need for recourse to such panicky and inconvenient conduct [55] . She not only had the conventional diplomatic network to hand with which to secure the best means of inoculation available abroad, but she also disposed of close counsel in the person of Nikita Panin (1718-83) her first minister, bereft of his fiancée – a victim of smallpox at Court – and trusted and knowledgeable advisers in Ivan Betskoy (1704-95) and Alexander Cherkasov (1728-88) and also a domestic medical service manned by many capable physicians and administrators. And her reach within the Russian empire was backed by her conviction that in so extensive a realm only autocracy could perform with the requisite activity and uniformity. [56] . It was Catherine’s own decision to set a signal personal example to invigorate inoculation in her Empire and the newly minted Suttonian inoculation lay to hand as the obvious tool. She used it with a will. It was not as if the Russian empire lacked eminently qualified and practised inoculators, but these men did not have the international prestige associated with the Suttonian method. The events surrounding her inoculation and that of her son-and-heir Paul were fraught and dramatic but she ensured that the achievement was magnificently publicised, celebrated and broadcast. The trial runs involving cadets had confused her inoculator, but such was her understanding of the procedure that she was able to overcome Dimsdale’s scruples and direct him to proceed in spite of everything. She fully deserved her triumph and made the most of it. Concurrently Ingen Housz had navigated not dissimilar anxieties and scepticism. The two inoculators never forgot their shared celebrity and remained friends for life, but Ingen Housz’s subsequent career was as a pioneering scientist and not – as Dimsdale’s – as a prominent protagonist of inoculation. He never published on the subject, in spite of having considered doing so on at least one occasion [57] [58] .
More than in Catherine’s case, Maria Theresa was stimulated by her own and her family’s bitter experience of smallpox [59] . As had Catherine, she made the decision, which in her situation was less easy because obstructed implacably by Anton de Haen (1704-76), at the summit of European medical repute, who in the tradition of his teacher Boerhaave (1668-1738) despised inoculation as an unaccountable and unscientific folk practice, not unrelated to witchcraft. De Haen believed in providing smallpox patients with the best treatment which could be offered in the event that the disease had not been avoided. Maria Theresa’s approach to the scene of Suttonian inoculation involved an official one through diplomacy and this it was − as we have seen − which stimulated the intervention of Pringle in his capacity as George III’s foremost, though by no means sole adviser, and the appointment to Vienna of Ingen Housz. In contrast to this, the appointment of a person to introduce Suttonian inoculation into Russia was − also as noted − made by the Russian Ambassador in London backed by a direct emissary from St. Petersburg [60] .
Closely concerned with the events of 1768 was Frederick II of Prussia. As his own first minister and as a man deeply interested in medicine, he had a decided view and wrote personally and reproachfully to Catherine, in response to her relation to him of the great success of her own inoculation, about what he considered to be the unjustifiable risk which she had taken [61] . Russian and British interest and diplomacy hoped that he would take a leaf from her book, but he appears to have summarily rejected the approach [62] . However a few years later Frederick took Suttonian inoculation on board from the physician William Baylies (1724-87), who had left England under a cloud but who was a capable operator and exponent of the method and who oversaw its initiation in Prussia [63] .
Elsewhere in Germany, with so many states to reckon with, it is not easy to summarise, but the substantial and ambitious campaign proposals of Johann Christian Wilhelm Junker (1761-1800) in the 1790s stand out in a prospect revealing rather less take-up of inoculation than in France [64] .
In France the introduction of Suttonian inoculation by a head of state was similarly delayed and only provoked by the catastrophe of Louis XV’s death from smallpox in 1774, immediately following which his successor Louis XVI was inoculated [65] . The French Royal inoculation was not, however, a signal of wholesale conversion to the method, but just one of a series of successes, which were often followed by further uncertainty and hesitation. It was only at the end of the century that a physician could publish his view that Suttonian inoculation had prevailed at last, after so much ebb and flow [66] .
In a Europe of many states there were also cases of heads of state undergoing inoculation with little or no effect on wider dissemination [67] . There had also been figurehead inoculations before 1768, but which had not provided anything like the spectacular impetus of the Russian and Austrian imperial ventures [68] .
Two features of inoculation campaigns emerged before 1768 and were re-emphasised in that year. The first was the practice of experiment on convenient controlled populations [69] , such as condemned prisoners, as in 1721 in London [70] , and most usually orphans or cadets. Ingen Housz inoculated orphans at the Foundling Hospital in London [71] and a specially assembled group of children in Vienna [72] while Dimsdale was provided with cadets in St. Petersburg, who, although reportedly indignant, had no choice in the matter [73] . Such inoculations were deemed to be essential precursors of the main event, and problems encountered on the way had to be resolved or rationalised, often in haste, before they took place.
The second feature of inoculation campaigns was the hospital. The London smallpox hospital at St. Pancras − half for smallpox patients and half for inoculation − was built by charitable subscription in 1746 and represented the latest purpose-built version of a series of establishments which had migrated around North London over the years [74] . It operated in an organised though limited way – relatively small numbers of patients for inoculation were involved − but its reputation attracted visits from physicians from other countries considering how best to exploit inoculation back home. A hospital came to be seen as central to any state inoculation campaign. In 1767 a large unused mansion was acquired to serve as an inoculation hospital prior to the St. Petersburg Imperial inoculation and was the first of several throughout Russia [75] , even including a purpose-built Siberian version near Irkutsk.
Signal adoption of Suttonian inoculation by a head of state was one thing, but the extent of its use was another. There were cases of landowners arranging for the inoculation of large households, estates or even entire villages [76] , but not many, and it seems that the kind of extension to all classes which had occurred earlier in Scotland and, following Daniel Sutton’s breakthrough, in England too, did not follow in European Russia. Indeed it is possible that smallpox posed less of a threat there than in the rest of the West. [77] But in another theatre an inoculation campaign was developed which was quite as exemplary and inclusive as was Girod’s in the Franche Comté. That Siberian peoples were particularly badly affected by epidemics was understood, and the Government’s reach and authority caused the organised inoculation of very large numbers of people, some of whom had themselves adopted inoculation as a folk practice [78] . The inoculation of Catherine II, her heir Grand Duke Paul and large numbers of the nobility in 1768/9 in St. Petersburg and Moscow led to the establishment of a government-supported campaign built on the Empress’s exploit, [79] backed by rules and regulations administered by the state, as well as government publicity of many kinds including the publication of Dimsdale’s book in Russian and another simplified version of his method adapted to Russian circumstances. [80] The large hospital which was established in St. Petersburg was followed by others elsewhere in the City as well as in Moscow and other urban centres, and - in time - beyond the Urals, paying special attention to native peoples, [81] this last as exemplified by the carefully planned hospital north of Irkutsk (Figure 6) which played its part in the regional campaign which achieved 15,380 inoculations between 1773 and 1779. [82] A. N. Radishchev, on his way to exile for nine years at Ilimsk, well to the north of Irkutsk, testified in a letter to Count A. R. Vorontsov from Tobolsk in July 1791 to the potential effectiveness of Russian inoculation campaigns when he wrote that ‘the grave can be closed to smallpox [by inoculation]’ in the context of an epidemic of measles which had given rise to many fatalities among children. Empress Catherine, twenty years before, had claimed that greater progress with inoculation was being made in Russia than in any other country. [83] The special hospital set up north of Irkutsk was designed to receive and process nomadic people undergoing inoculation [84] . The Governor was responsible for the campaign and was served by Russian and German administrators and physicians [85] .
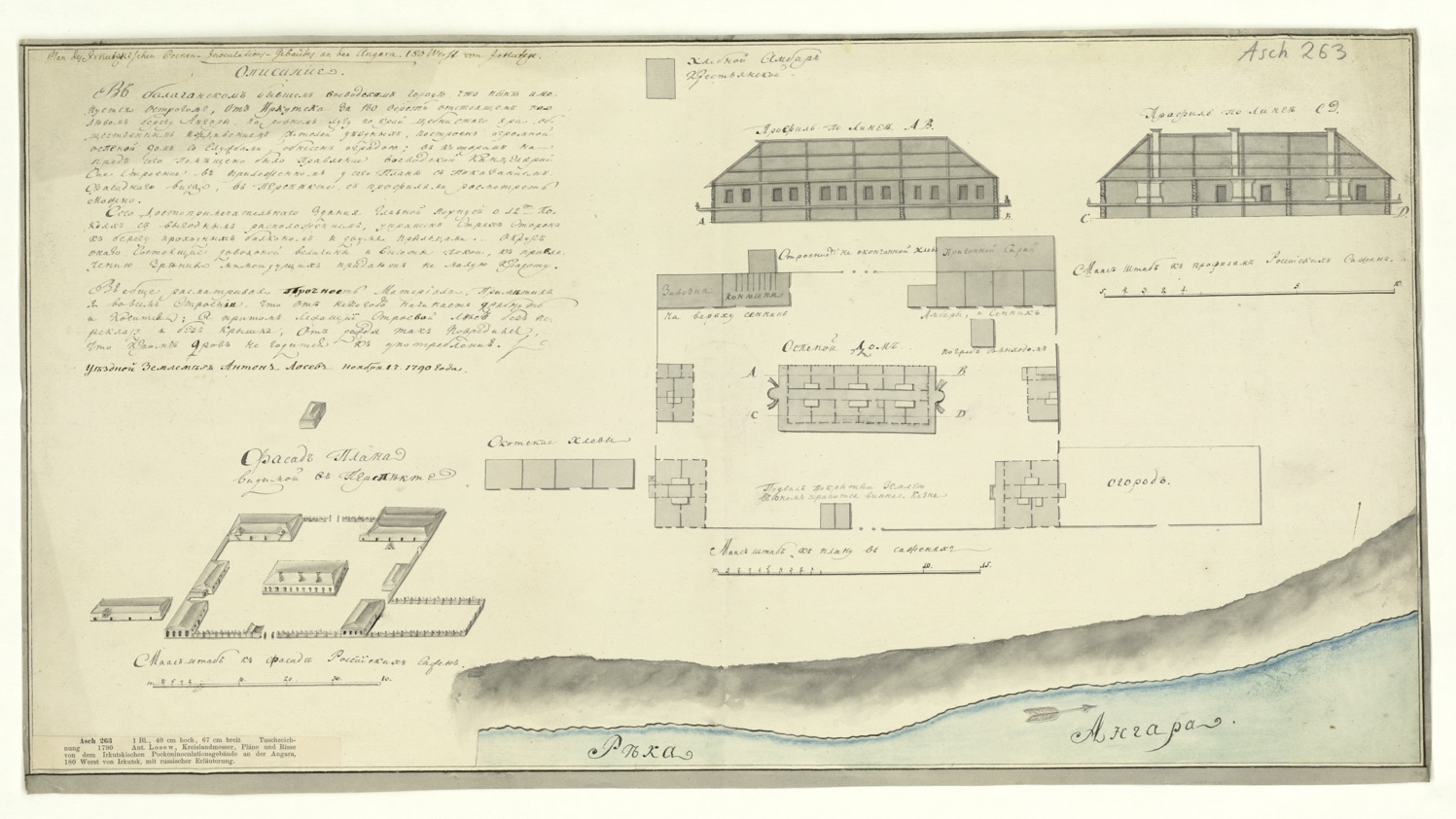
Figure 6: Inoculation hospital on the Angara River 180 versts from Irkutsk. SUB Göttingen, Cod. Ms. Asch 263
The limitations of the London Hospital came to be seriously debated in the 1770s. In 1776 John Watkinson (fl.1777) published a case in support of a campaign for inoculating the poor in their homes [86] . He drew on other European opinion and revealed in so doing that there was widespread support for his case and that the embargo on inoculation in existence in numbers of cities and towns acted to exclude the urban poor from the benefits of inoculation. An alarmed and by then powerful medical authority, Dimsdale weighed in against Watkinson’s idea because of the certainty, as he saw it, that inoculated people were bound to remain in circulation and so pass the disease to those who had never had smallpox, often with fatal consequences. A supporter of hospitals, Dimsdale had described an opportunity for enlarging the St. Pancras smallpox hospital [87] which was never in the event taken up. His case against Watkinson − published and circulated in coffee houses − although with little support from other authorities [88] , was a strong indictment stressing the increased number of deaths which he saw as bound to ensue from inoculating the poor in their homes [89] . Both Dimsdale and his opponents used statistical evidence to support their cases without being able to obtain any convincing advantage [90] . John Lettsom (1744-1815), a Dissenter and successful physician and a moving spirit behind the campaign to inoculate the poor sprang into the lists in defence of Watkinson and − as an experienced controversialist [91] − attacked Dimsdale forcefully and to damaging effect, holding him up to ridicule as a person without proper qualification, knowing neither Latin nor any other language than English, in complacent enjoyment of enormous income and dubious foreign honours and prepared himself to inoculate the rich in their urban homes very profitably but not the poor [92] [93] . At one point Lettsom, as part of his campaign got himself invited to a lunch at Dimsdale’s house at Hertford attended by the Russian Ambassador. Having been to it he then succeeded in causing Dimsdale great offence by publishing what appeared to be an account of the private occasion [94] . Lettsom’s gibes provoked further exchanges and other physicians joined in on his side. A well written and even-handed but anonymous contribution on the whole favourable to Dimsdale’s case may have had little effect [95] . Eventually Dimsdale desisted and later appeared to acknowledge that there was something to be said after all in favour of a campaign to extend inoculation so as to embrace cities as advocated by Lettsom and his supporters [96] . Dimsdale’s case was weakened by the lack of interest on the part of the Smallpox Hospital Trustees in extending the building. Nor, in spite of his expectations and being himself a well-connected Member of Parliament from 1780 to 1790, was any Parliamentary or governmental support forthcoming for such a project [97] [98] . His contention that un-inoculated bystanders who had never had the natural smallpox could and would be infected and killed was incontrovertible, and Watkinson’s supporters struggled when confronted with actual cases in point. But Dimsdale’s reading of how the London poor lived − while accurate − did not result in the disastrous consequences which he foresaw, and on the whole the virus proved un-infective [99] . For him, one death was too many, while for his opponents – although they could not say so – a few deaths were more than counterbalanced by inoculation of the poor carried out on a substantial scale. Thus inoculation became generalised in much of England in the sense that it became, potentially at least, an option available to all.
If the provision of large hospitals dedicated to smallpox and inoculation faded, private hospitals for inoculation did not. First employed in 1749 in England [100] they were also met with frequently in the British North American settlements [101] . Such an inoculation house was central to Daniel Sutton’s breakthrough to a wide public at Ingatestone and also to Dimsdale’s practice at Hertford. It is likely, however, that the periodic town and village inoculations which became almost routine depended mostly on ad hoc arrangements rather than private inoculation hospitals [102] . In village, market town and city inoculation can be seen as gradually establishing itself by differing means, always within or alongside the rough and ready framework of the Old Poor Law [103] .
The Dimsdale/Lettsom public dispute marked the confused beginning of inoculation’s availability to a wider cross-section of the public. It also re-asserted to some extent the importance of the practical operator. A practice which had emerged as folklore had been exploited not only by physicians such as Tissot and Gatti but also by surgeons, apothecaries and quite unqualified persons of many kinds. Indeed the Suttons themselves typified this trend, as did Dimsdale – trained at St. Thomas’s hospital, but a son and grandson of unqualified practitioners and who had himself purchased his Aberdeen qualification. Lettsom’s engagement with the issue can be seen as a renewed acceptance of inoculation as much on moral as on scientific grounds, by a new medical cadre which owed much to Scottish universities, with a dash of English Dissent.
Suttonian inoculation had fallen on fertile ground in Ireland and Daniel Sutton’s franchising system was put into operation there, greatly augmented among scattered rural populations by unqualified operators including priests. [104] Transmission in print of Suttonian practice came later to Spain and Portugal than to the rest of Europe, but when it did it was – in the case of Spain – the work of the Irishman Miguel O’Gorman (1749-1814). Having been sent to London to learn Suttonian inoculation he did much to break down resistance to the operation at Madrid and later practised it in the new world at Buenos Aires. [105] This presaged a dramatic enlightened response and campaign by Spanish Imperial authorities in defence of the Maya of Guatemala, that of José Flores (1751-1824) from 1780 onwards, which culminated in a major seaborne expedition to introduce first inoculation and then vaccination to much of the empire. [106] Flores’s method of inoculation − using Cantharides – designed to counter the Maya’s fear of the lancet, was an ingenious adaptation to local conditions.
Like Spain, both France and Britain assumed involvement and responsibility in the New World. The New England colonists famously learned that some of their slaves – originating from West Africa – were familiar with the concept [107] , and inoculation was as widely known as it was back in Britain. At the time of the Suttonian breakthrough, Kirkpatrick (Kilpatrick) (1696-1770), who was an American writer, counted as the best exponent of inoculation writing in English, so that – as in Scotland – systematic exploitation of inoculation pre-dated the Suttonian surge, which manifested itself nevertheless in print and practice when it came. Actual and potential outbreaks of smallpox among armies caused leaders to insist sometimes on quarantine and on other occasions on inoculation on Suttonian lines to avoid repetition of disasters experienced by the colonists in their bid for independence [108] .
In the Caribbean both French and English regimes inoculated slaves of West African origin wholesale in order to protect the productive capacity of their sugar plantations. Again, we are dealing with a population already supportive of and familiar with the concept and there was no attempt made to apply all the early aspects of Suttonian inoculation, and preparation in particular was not featured. There was a Suttonian link between the Caribbean and Europe in the form of Daniel Sutton’s father-in-law Siméon Worlock, who having learned the trade in St. Domingue [109] moved to France to become one of the most prominent Suttonian inoculators there [110] .
The native American populations were just as vulnerable to epidemic smallpox as the Siberian peoples but in the confusion of civil war they had little chance of protection, and on the contrary were, on at least one occasion, purposely infected with smallpox to neutralise them – a startling contrast between the exercise of Russian and British rule, prefiguring further and greater disasters for native North Americans in uneasy association with the newly independent colonists [111] .
British successes in India led to another encounter with folk inoculation, which had been developed by Hindus, who equated smallpox with a goddess – Sitala – to be placated like the Georgian ‘batonébis’ at all costs. This facilitated the task of administrators in the Madras Presidency who were using European inoculation, although their imported technique was sometimes met with suspicion and resistance [112] .
China appears to have been unaffected by Western inoculation. It had a very strong tradition of its own from the seventeenth century, particularly in the south and it experienced − quite independently of the West − many of the developments discussed here, including imperial example: the emergence of inoculators unconnected at first with the medical profession: the striving for attenuation and the shortcomings of quarantine [113] .
The introduction of Suttonian inoculation to Europe and thence to the empires then dependent upon it [114] – sudden and top-down at first but later more gradual – was at no time unaccompanied by a bottom-up impetus, tending through its independent workings to define and establish its place in peoples’ lives. Fear was the emotion which stimulated responses – fear of death or of disfigurement, and fear of disruption of life’s familiar social and economic patterns. The fear was not continuous but recurrent and intense when related to the periodic onset of epidemics, and it was this which most often forced acceptance of inoculation on those who instinctively feared it. And broadcast knowledge of Daniel Sutton’s breakthrough braced the collective resolve of hitherto unimaginable numbers of people in every walk of life, promising the possibility of salvation for everyone. Where smallpox was endemic – a steady toll rather than mass destruction – familiarity to an extent bred contempt, but the fear, although it was less peremptory, was nevertheless intolerable and the chance of protection from the disease was not to be passed up on account of some scruples concerning collateral damage. The motives of those who offered or decreed the remedy of inoculation ranged from the downright commercial to the disinterested, but throughout the spectrum, trade and generosity were usually present in varying proportions in every intervention. Paternalism and Enlightenment [115] kept company with mercantilist ambition and entrepreneurial flair co-habited with the rights of man. The advent of Suttonian inoculation created the possibility of a step change from the numerically and socially limited episodes which it superseded.
If Robert Sutton supplied a practical technique, Daniel attached a secret ingredient and the ambition and organising ability to make it available to thousands, both directly and through franchising. In so doing he ably profited from his offer of a providential solution and – assisted by the scale of his operations – did so at a reduced cost, and sometimes even for free. He made spectacular headway. A few attempts to patent parts of the process had failed before [116] , but he met with notable success, and in so doing – in England certainly – must take the credit for placing lifelong immunity within the reach of an entire population. Before the Suttons, the profits of the then much more limited market had been largely monopolised by doctors, with their equivalent of Daniel’s secret medicine in the form of unnecessarily lengthy preparation. This trade – though diminished – survived the introduction of Suttonian inoculation and – like that of the Suttons – often, in emergencies, tempered the wind to the shorn lamb, sometimes backed by charitable local impulse to augment the poor rate.
The British Crown, ministries and Parliament were not actors in this vital matter of public health at home, but in several other countries, in particular Sweden [117] , Denmark and Norway [118] , Holland, the Genevan Republic and Switzerland governments backed and sometimes initiated and sustained inoculation campaigns. In a few cases their ambitions were manifested before Daniel Sutton’s Essex breakthrough, but all involved were stimulated by that event and availed themselves of the codification and guidance available to them in translation.
In the broad debate on medicalisation [119] where do the decades of Suttonian inoculation fit? Are they a part of the introduction of scholarly medicine to a cross-section of the population [120] ? Do they represent not just the exposure of everyman to ever more comprehensive medical controls from above, but to a set of norms appropriate to the understanding of various social classes [121] ? Or do they bear witness to the hegemonic imposition of elite medicine as one of many prongs of a wider programme of the neutralisation or suppression of village culture [122] ? It is perhaps safest to see Suttonian inoculation as an independent phenomenon operating more or less powerfully and independently of nascent medicalisation and presenting so tempting a benefit to all social classes as to provoke a variety of governmental and societal responses. It could not be and was not ignored − at least not for long – but irresistibly forced the pace of medical care from above as well as from below. On the other hand its successor, vaccination – implemented on a vast scale – was clearly a formidable ingredient of medicalisation, however defined.
An essay about the introduction and spread of a form of smallpox inoculation cannot avoid inclusion of some reference to the consequence in terms of demographic history, if only to note that the once favoured doctrine that inoculation underpinned population growth in England to an extent which facilitated the Industrial Revolution has given way to a far more complex account featuring improving general health and sanitary conditions and the downgrading, indeed elimination, of the activities of doctors as a factor promoting increase of population [123] .
So inoculation should now be viewed as solace, certainly, but as one only of many factors operating to reduce the death rate, itself of less significance than earlier marriage and consequently birth rate. What remains important is that an ancestral fatalistic attitude with regard to an epidemic disease as viewed by the Mingrelians had first been modified in a possibly random scatter of populations around the world through folk inoculation and then, by the close of the eighteenth century, virtually supplanted everywhere by an understanding that salvation could and should be made universally available thus propelling an enlightened idea of rights into the fog of fatalism.
Arnold Klebs concluded in 1913 that: ‘Plentiful suggestions are to be found everywhere which lead one to infer that variolation (inoculation) without vaccination might have furnished the world with an equally safe and perhaps more efficient method of preventive immunisation.' [124] His aim then had been ‘… rather to open avenues for future research than to give a complete and detailed account of the more important phases’ of the course of [inoculation] ‘through the civilised world of the eighteenth century’. His purpose as a doctor was a medical one and a historian [125] writing in 1957 noted this while claiming for historians the duty of examining the issue more comprehensively, and there has indeed been a steady flow of findings since then both on the reception of inoculation: its implementation, and the demographic consequences. Among recent examples relating to the previously unrecognised extent of inoculation one may include France [126] , England [127] , Scotland [128] , Scandinavia [129] , Prussia [130] , Germany [131] , Russia [132] and India [133] − all included in the bibliography below − and debate on the demographic, social and economic consequences for England as contrasted with Europe has continued for decades, but even so it must be suspected that many gaps remain in any account of how far inoculation had become the norm by the end of the eighteenth century. As the issue has been scrutinised country by country, people by people and language by language an impression is borne in that each investigation has tended to support the idea that inoculation – particularly Suttonian inoculation – was more prevalent than had been previously recognised and that further research is likely to provide further confirmation of this state of affairs, and also of the likelihood that – as with folk inoculation – the remedy was adopted on a scale only to be indicated rather than proved. Even so a pattern emerges of more or less implementation of inoculation tending to the better understanding of the reasons for such contrasts, sometimes highlighting that some countries, including England, which adopted inoculation most effectively were slowest to insist on vaccination [134] and others, particularly Spain – a latecomer to inoculation – were to the forefront by the end of the century, at least insofar as empire was concerned, and − post Jenner – substituted vaccination for inoculation almost immediately.
The Suttons − principal actors in the fight against smallpox at the time – and who gave their name to the operation, may have done well enough out of their endeavours [135] . Dimsdale’s attitude to Jennerian vaccination, the triumph of which he lived to see, is not recorded, but by the time of his death at his home in Hertford in 1800 he had come to be associated with much that was outdated [136] . Ingen Housz broke cover near the end of his life to bring Jenner to order for the methodological shortcomings – as noted by a distinguished pioneer scientist − of his great paper [137] . Girod died full of honours at his home village – Mignovillard − where to this day he has not been forgotten. George Hodges, whose death from smallpox at Little Berkhamsted was the only one experienced during the midwinter inoculation there in 1768, stands in through an historical accident [138] as a named ‘unknown warrior’ for the numberless unrecorded children worldwide who became the principal victims of the scourge, which itself now has an afterlife in – it is to be hoped – only two places, both high-security laboratories.
'About the beginning of the Year 1768 George Hodges (he was buried Febr 12th) a youth of 10 yrs of age was taken desperately ill; His Parents imagined, but did not know it was the Small Pox; after being ill some days they waited upon Mr since Baron Dimsdale for his advice; who readily came in the evening, tho the snow was above a foot deep and his servant got a dangerous fall; He insisted upon me going with him to the Patient We found him in a sad situation full of dirt and sores. The Doctor with a humanity peculiar to himself washed him, removed all nasty obstructions and by his care preserved his life some days upon our return to the Parsonage he told me it was the Small Pox of the worst sort the infection of which wou[l]d certainly go thro the Parish, but if I and the Parish choose it he would inoculate the whole gratis in two days. Immediately used w[h]ich persuasions I cou[l]d; many complied with great cheerfulness and the rest seeing they cou[l]d not prevent the Inoculation taking place, soon came into it, all succeeded and did well: he kindly gave them medicine and attendances Doctor Engen:house; afterwards Physician to the Empress Queen and who inoculated all her Family was for the purpose of experience attending upon Dimsdale. The Inhabitants of Bayford upon seeing our People so cheerfully enter upon it beg’d of the Dr at the same time to exert the same charity to them: their request was complied with, and they did well. ... '
Acknowledgements
My sincere thanks to Roger Bartlett and Elena Marassinova, whose help with this project has been very much appreciated and who bear no responsibility for any remaining errors in the final text.
Footnotes
[1] In this I follow the argument advanced in Genevieve Miller, The Adoption of Inoculation for Smallpox in England and France, (Philadelphia, PA, 1957), Preface p.2.
[2] T. Sakhokia, ‘Le culte de la petite vérole en Géorgie. Une page de la médecine populaire’, Bulletins et Mémoires de la Société d’anthropologie de Paris,Ve Série, 4 (1903), p.262.
[3] It has been suggested that smallpox ‘was perhaps unique in that specific deities associated predominantly if not exclusively with smallpox were found in all major regions of the Old World’: C. S. McClain, ‘A new look at an old disease: Smallpox and Biotechnology’, in M. C. Inhorn and P. J. Brown (eds.), The Anthropology of Infectious Disease: International Health Perspectives (Amsterdam, 1997), pp.103-4.
[4] Sakhokia, ‘Le culte de la petite vérole en Géorgie’, pp. 262-275.
[5] Possibly including the Mingrelians.
[6] A. C. Klebs, ‘The historic evolution of variolation’, Bulletin of the Johns Hopkins Hospital, 265 (1913), pp. 69-71 remains an effective summary. A contemporary counterpoint for the New World including a list of peoples not yet affected by epidemic smallpox was offered by J. J. Paulet, Histoire de la Petite Vérole … (Paris, 1768), pp.27-9.
[7] The principal smallpox virus.
[8] Many eighteenth-century discussions of inoculation were prefaced by a list of the various parts of the world from which folk inoculation had been reported. Many such were copied from earlier texts but the overall totals were impressive. Modern discussions include those of William. H. McNeill, Plagues and Peoples, (Oxford, 1977) and McClain, A new look at an old disease (see fn.2 above).
[9] Miller, The Adoption of Inoculation, pp.48-52.
[10] Edward Jenner, An Inquiry into the Causes and Effects of the Variolae Vaccinae, a disease discovered in some of the western counties of England, particularly Gloucestershire, and known by the name of the Cow Pox (London, 1798).
[11] F. Fenner, D. Henderson, I. Arita, Z. Ježek, I. D. Ladnyi, Smallpox and its Eradication (Geneva, 1988), p.1249.
[12] The cold method. Exposing the patient to fresh air. The English Physician Thomas Sydenham (1624-1689) was its best known advocate.
[13] D. Van Zwanenberg, ‘The Suttons and the business of inoculation’, Medical History, 22 (1978), pp.73-5; J.R. Smith, The Speckled Monster: smallpox in England, 1670-1970, with particular reference to Essex, (Chelmsford, 1987), p.41.
[14] Humoral medicine. As exemplified by the use of mercury and the many pre-inoculation diets prescribed.
[15] For Gatti’s career, see A.C. Klebs, ‘The historic evolution of variolation’, pp.79-82; and A.C. Klebs, Die Variolation im achtzehnten Jahrhundert, (Giessen, 1914), pp.25, 37-42, 61-2.
[16] T O’Scanlan, Practica moderna de la Inoculacion, con varias Observaciones y Reflexiones fundadas en ella, precededas de un Discurso sobre la utilidad de esta operacion, y un Compendio Historico de su origen, y de su estado actual, particularmente en Espana; con un Catalogo de algunos Inoculados (Madrid, 1784).
[17] Smith, The Speckled Monster, pp.72 and 79-80; W. Woodville, The history of the inoculation of the small-pox in Great Britain, vol. 1 (London, 1796), pp.349-50.
[18] Robert Houlton (1738/9-1815). Author of Indisputable facts relative to the Suttonian art of inoculation (Dublin, 1768).
[19] T. Dimsdale, The Present Method of inoculating for the Small-Pox (London, 1767).
[20] A. Klebs, Die Variolation im achtzehnten Jahrhundert: Ein historischer Beitrag zur Immunitätsforschung’ (Giessen, 1914) p.41.
[21] For an account of inoculation in this period see M. Nicoli, ‘La bataille du siècle. Défenseurs et détracteurs de l’immunisation variolique dans le Journal Helvétique', in S. Huguenin & T. Léchot (eds.), Lectures du Journal helvétique 1732-1782 (Geneva, 2016), pp.293-314.
[22] By the Faculty of Medicine at the Sorbonne, first instructed by the Parlément in 1763.
[23] A. Munro, An Account of the Inoculation of Small Pox in Scotland (Edinburgh, 1765). Cited in D.Brunton, ‘Smallpox inoculation and demographic trends in eighteenth-century Scotland’, Medical History, 36 (1992), pp.87-9.
[24] La Duchesse de Boufflers, who had been inoculated by him two years previously came down with smallpox. C. Seth, Les rois aussi en mouraient: Les Lumières en lutte contre la petite vérole (Paris, 2008), p.65.
[25] Klebs, Die Variolation im achtzehnten Jahrhundert, p. 41.
[26] C. Seth, Les Rois aussi en mouraient. Les Lumières en lutte contre la petite vérole (Paris, 2008), pp.87, 97.
[27] A. Klebs, Die Variolation im achtzehnten Jahrhundert, p.32.
[28] The opinion of his Majesty’s Physicians and Surgeons, given Jan. 23, 1768, in regard to Messrs Sutton’s practice in Inoculation, in consequence of a Letter from Sir John Pringle, dated London, May 6, 1767, to Mr Brady at Brussels; and another from Count Kaunitz Rittburg, dated Vienna, December 17, to Count Seilern, ambassador from the Empress Queen to the King of Great-Britain. London, 23 Jan. 1768.
[29] The source for Pringle’s detailed knowledge of Sutton’s, Dimsdale’s and Ingen Housz’s practices at that time is his partially indexed ‘Medical Annotations’ at the Edinburgh Royal College of Physicians.
[30] For an account of Ingen Housz’s life and work see N. and E. Beale, Echoes of Ingen Housz, the long lost story of the genius who rescued the Habsburgs from smallpox and became the father of photosynthesis, (Salisbury, 2011).
[31] O. Sonntag (ed.), John Pringle’s Correspondence with Albrecht von Haller (Basel, 1999), p.109.
[32] Little Berkhamsted and Bayford.
[33] The town and country magazine or universal repository of knowledge, instructions and entertainment. 1769, p.309. Cited by P. H. Clendenning, ‘Dr. Thomas Dimsdale and Smallpox Inoculation in Russia’, Journal of the History of Medicine and Allied Sciences, 28 (1973), p.118.
[34] R. Hingston Fox, Dr. John Fothergill and his friends, (London, 1919), pp.86-7.
[35] Maria Theresa acknowledged the King’s ‘most tender sentiments’ and ‘compassion’. Vienna. Österreichisches Haus-Hof-Staatsarchiv (England Section) F:157, Letter from Prince Kaunitz, Vienna, to Count Seilern, London 4 March 1768. Cited in Beale, Echoes of Ingenhousz, pp.108-9.
[36] Although it gave the King ‘… great pleasure to find, that [inoculation was] to be introduced into the Empress of Russia’s dominions’ he could ‘not avoid feeling great anxiety from the reports of [Empress Catherine’s] intentions to submit to the operation; … .’ Sbornik Imperatorskogo Russkogo istoricheskogo obshchestva (hereafter SIRIO), XII (1878), 203. Letter from Viscount Weymouth to Lord Cathcart, St. James’s, 18 October 1768.
[37] Krünitz, Verzeichnis der vornehmsten Schriften von den Kinderpocken und deren Einpfropfung, (Leipzig, 1768). Although many of the later re-prints recorded by Krünitz have not been included in figures 1-5 the overall trends which the figures demonstrate should not be much affected.
[38] F. Olberg, Beiträge zur Litteratur der Blattern und deren Einimpfung, vom Jahre 1768 bis 1790 (Halle, 1791).
[39] Between 1767 and 1793, Dimsdale’s book − ‘The Present Method … .’ – ran to eight English language editions, including six in London, one in Dublin and another in Philadelphia. There were also three translations each into French, German and Italian, and one each into Dutch, Swedish, Russian and Portuguese.
[40] Table 1 includes some titles not included with those used to compile Figure 1.
[41] Modern geographical expressions and nations are employed to define ‘country’.
[42] Salomon Schinz, (1734-84), Swiss (Zürich) physician.
[43] Best described in B. Anderson, Imagined Communities: Reflections on the Origins and Spread of Nationalism (London & New York, 1983).
[44] Klebs, Bibliography of variolation.
[45] Klebs, ‘The historic evolution of variolation’.
[46] Klebs, Die Variolation im achtzehnten Jahrhundert.
[47] Klebs, ‘The historic evolution of variolation’, p.83
[48] An account of the Franche Comté inoculations is provided by P. Darmon, La longue traque de la variole (Paris, 1986), pp.127-36.
[49] Darmon, La longue traque, p.128
[50] Ibid.
[51] La Société royale de médecine.
[52] Beale, Echoes of Ingen Housz, p.131.
[53] T. Dimsdale, Il Presente Metodo d’innestare il Vajuolo Al quale sono aggiunti Alcuni sperimenti, istituiti colla mira di scoprire gli effete d’una somigliante condotta nel Vajuolo Naturale del Dottor Tommaso Dimsdale, Tradotto in Italiano dalla terza edizione di Londra: Con alcune Osservazioni, e Note del Signor Tommaso Houlston Medico Inglese (Naples, 1768).
[54] H. Foucquet, Traitement de la Petite Vérole des Enfans, auquel on a joint La Méthode actuelle d’inoculer la Petite Vérole … (Amsterdam et se trouve à Montpellier, 1772); T. Houlston, ‘Lettre sur les Ravages de la petite-Vérole à Montpellier, & sur l’inoculation’, Journal de Médecine, Chirurgie, Pharmacie, &c. Février 1771, 35 (Paris, 1771), pp.131-40.
[55] J. Alexander, Catherine the Great: Life and Legend, (Oxford, 1989), pp.145-6.
[56] Catherine II, Instructions adressées par Sa Majesté L’Impératrice de toutes les Russies à la Commission établie pour travailler à l’exécution du projet d’un Nouveau Code de Loix, (Yverdon, 1769), p.8.
[57] Beale, Echoes of Ingen Housz, pp.260-1, 269, 288, 310.
[58] Ingen Housz’s detailed notes – sent to Pringle over a period of time on various aspects of the Little Berkhamsted inoculation – indicate his close interest and understanding. Pringle, ‘Medical Annotations’.
[59] An account of the Habsburg inoculations is provided by Beale, Echoes of Ingen Housz, pp.92-174.
[60] Clendenning, Dr. Thomas Dimsdale, pp.117-9.
[61] SIRIO, XX, 47. Letter from Frederick II to Empress Catherine, 26 November 1768.
[62] Clendenning, Dr. Thomas Dimsdale, p.126.
[63] A.C. Klebs, ‘The historic evolution of variolation’, in Bulletin of the Johns Hopkins Hospital, 265 (1913), p.77; M. Sonntag, Pockenimpfung und Aufklärung (Bremen, 2014), p.199.
[64] A-H. Maehle, ‘Conflicting Attitudes Towards Inoculation in Enlightenment Germany’, in R. Porter (ed.), Medicine in the Enlightenment (Amsterdam and Atlanta, GA, 1995, pp. 198-222); M. Sonntag, Pockenimpfung und Aufklärung: Die Popularisierung der Inokulation und Vakzination: Impfkampagne im 18. und frühen 19. Jahrhundert (Bremen, 2014), pp.251-264.
[65] P. Darmon, La Variole, les Nobles et le Princes (Paris, 1989), pp.85-146.
[66] F. Dezoteux & L. Valentin, Traité historique et pratique de l’inoculation (Paris, L’an 8 [1799]), pp.82-92.
[67] 1777 Naples. Seth, Les rois aussi en mouraient, p.158.
[68] 1760 Denmark. O’Scanlan, Practica moderna, p.397.
[69] Such populations could themselves be prone to epidemic disasters, as was the Moscow Foundling Hospital not long before Empress Catherine’s inoculation. See A. Renner, Russische Autokratie und europäische Medizin. Organisierter Wissenstransfer (Stuttgart, 2010), p.131.
[70] S. Williamson, The Vaccination Controversy (Liverpool, 2007), pp.28-39.
[71] Beale, Echoes of Ingen Housz, pp.80-7.
[72] Ibid. pp.139-40.
[73] T. Dimsdale, Tracts on Inoculation, Written and published at St. Petersburg in the year 1768 … (London, 1781), pp.20-3.
[74] S. Williamson, The Vaccination controversy, pp.51-3.
[76] Two examples. Dimsdale’s inoculation for the Quaker Hanburys at Great Coggeshall in 1768. J.R. Smith, The Speckled Monster, p.80, and of Grigorii Orlov’s estates at Ropsha and Kipen near St.Petersburg in the same year. R. Bartlett, ‘“Ropsha, where Peter III was murdered …”: Faces and Façades of an Imperial Estate’, in S. Dixon, (ed.), Personality and Place in Russian Culture. Essays in Memory of Lindsey Hughes (London, 2010), pp.169-70.
[77] A.L. Von Schlözer, Von der Unschädlichkeit der Pocken in Russland und von Russlands Bevölkerung überhaupt, (Gotha und Göttingen, 1768). His (contested) hypothesis was that the widespread popular use of steam baths conferred some protection from smallpox. For another contemporary discussion see W. Tooke, View of the Russian Empire during the reign of Catherine the Second and to the close of the eighteenth century, Second Edition edn. (London, 1800), vol. 1, pp.546-8.
[78] Tooke, View of the Russian Empire, vol. 2, p.87. Tooke stated that further east the ‘Kamtshadales’ too inoculated themselves. Ibid. p. 89.
[79] H. Storch, Historisch-statistisches Gemaelde des Russischen Reichs am ende des achtzehnten Jahrhunderts. Part 1 (Riga, 1797), p.425; V. O. Gubert, Ospa i Ospoprivanie(St Petersburg, 1896), vol. 1, pp.223-56; Renner, Russische Autokratie, pp.134ff.
[80] T. Dimsdale, Nyneshniĭ sposob privivat' ospu … (SPb 1770); Kratkoe i iasnoe nastavlenie, kakim obrazom' soderzhat' bol'nago kak v natural'noi, tak i v privivnoi ospe po metodu Gospodina Barona Dimsdalia (SPb, 1770).
[81] Gubert, Ospa i Ospoprivanie, vol. 1, pp.121-5; A. C. Klebs, Die Variolation im achtzehnten Jahrhundert, p.57.
[82] Although by 1790, the year when the installation was recorded, it was described as unusable and fit only for firewood, the remarkable figures for Irkutsk are for the 1770s: Gubert, Ospa i ospoprivivanie, vol. 1, p.254.
[83] SIRIO, XIII, p.127. Letter from Empress Catherine II to Thomas Dimsdale. 8 July 1768 Old Style.
[84] Surveyor Anton Losev’s 1790 drawing shows and describes a fenced area of a little over 4,500 square metres, containing the main inoculation campaign building, with enough sufficiently well-aired rooms to constitute an inducement to local peoples: arrangements for animal fodder: a granary: a bakery: stables with hay storage above: underground storage, and a vegetable garden. The main building − he notes − being of some beauty as well as utility.
[85] Cf. the Barons Von Asch, father and son and Renner, Russische Autokratie, pp.65-86.
[86] J. Watkinson, An Examination of a Charge brought against Inoculation by De Haen, Rast, Dimsdale and other Writers (London, 1776).
[87] T. Dimsdale, Thoughts on General and Partial Inoculations (London, 1776), pp.57-61.
[88] R. Walker, An Inquiry into the Small-Pox, Medical and Political … (London, 1790) was a late entry – not in favour of inoculating the poor in their homes − indicating that the debate still continued.
[89] T. Dimsdale, Observations on the introduction to the plan of the Dispensary for General Inoculation. With remarks on a Pamphlet, entitled, “An Examination of a Charge brought against inoculation by De Haen, Rast, Dimsdale, and other Writers. By John Watkinson, M.D.” (London, 1778).
[90] A. Rusnock, Vital Accounts: Quantifying Health and Population in Eighteenth-Century England and France (Cambridge, 2002), pp.92-108).
[91] A notable target had been the renowned uroscopist Dr. Theodor von Myersbach. For this exchange see R. Porter, ‘ “I think ye both Quacks”: The controversy between Dr Theodor Myersbach and Dr John Coakley Lettsom’, in W. Bynum & R. Porter, (eds) Medical Fringe and Medical Orthodoxy 1750-1850 (Croom Helm, 1987).
[92] J. Lettsom, A Letter to Sir Robert Barker, Knt. F.R.S. and George Stacpoole, Esq; upon General Inoculation (London, 1778).
[93] Word had got out of a failure of quarantine during two of Dimsdale’s inoculations of the Moscow nobility. Anon, A letter to J. C. Lettsom M.D. F.R.S. S.A.S &c. … by an uninterested spectator of the Controversy between Baron Dimsdale and Dr. Watkinson … (London, 1779), p.33.
[94] J. C. Lettsom, Observations on Baron Dimsdale’s remarks on Dr Lettsom’s letter to Sir Robert Barker & George Stacpoole Esq respecting General Inoculation (London, 1778).
[95] Anon, Considerations on the propriety of a plan for inoculating the poor of London at their own habitations … (London, 1779).
[96] W. Black, Observations medical and political on the small-pox and inoculation… Appendix to the first chapter… (London, 1781), p.2.
[97] J. Innes, Inferior Politics: Social problems and Social Politics in Eighteenth-Century Britain, (Oxford, 2009), pp.21-47, 78-108.
[98] Jonas Hanway (1712-1786) agreed with Dimsdale that Parliament should intervene but in this case may have made no progress. J. Hanway, The Defects of Police (London, 1775), pp.89-92
[99] The reasons for this un-infectivity in London − whether due to increased inoculation or to reduced mortality from endemic smallpox rendering it a disease primarily of childhood – are discussed in P. Razzell, ‘The decline of adult smallpox in eighteenth-century London: a commentary’, The Economic History Review, 64, 4 (2011), pp.1315-1335.
[100] Thomas Frewen (1704-91) at Rye, Sussex in G. Miller, The Adoption of Inoculation, p.165.
[101] E. Fenn, Pox Americana. The Great Smallpox Epidemic of 1775-82 (Stroud, 2004), p.24.
[102] D. Brunton, ‘Pox Britannica: Smallpox inoculation in Britain, 1721-1830’ (unpublished PhD thesis; University of Pennsylvania, 1990) pp.143-150.
[103] For villages and market towns, see R. Dimsdale, ‘The Old Poor Law and medicine in and around Hertford, 1700-1834', in S. King and G. Gear (eds), Social Welfare in Hertfordshire from 1600. A Caring County? (Hatfield, 2013), pp.27-30.
[104] P. Razzell, The Conquest of Smallpox: The Impact of inoculation on Smallpox Mortality in Eighteenth-Century Britain (Firle, 1977).
[105] T. O’Scanlan, Practica moderna, pp.LXXIX-LXXXI.
[106] M. Few, ‘Circulating smallpox knowledge: Guatemalan doctors, Maya Indians and designing Spain’s smallpox vaccination expedition, 1780-1803’, British Journal for the History of Science, 43, 4 (2010), pp.519-37.
[107] For Cotton Mather and Onesimus, see fn.54 above.
[108] Fenn, Pox Americana, pp.31-2; J. Morgan, A Recommendation of inoculation according to Baron Dimsdale’s method (Boston, 1776).
[109] Haiti.
[110] K.K. Weaver, Medical Revolutionaries: the Enslaved Healers of Eighteenth-Century Saint Domingue (Chicago, 2006), p.52. Warlock (or Worlock), from Antigua, carried out large scale inoculation on St. Domingue before moving to Paris: see J. Quier, ‘A letter from Mr. John Quier, practitioner of physic in the island of Jamaica, to Dr. D. Monro, Jermyn-street, London, on the Small-Pox and Inoculation’, Letters and essays on the Small-Pox and inoculation, the Measles, the dry belly-ache, the Yellow, and remitting, and Intermitting Fevers of the West Indies (London, 1778), pp.1-104.
[111] E. Fenn, ‘Biological Warfare in Eighteenth-Century North America: Beyond Jeffery Amherst’, The Journal of American History, 86, 4 (2000), pp.1555-7.
[112] N. Brimnes, ‘Variolation, Vaccination and Popular Resistance in Early Colonial South India’, Medical History, 48, 2 (2004), pp.199-228.
[113] C-F. Chang, ‘Aspects of smallpox and its significance in Chinese history’ (unpublished PhD thesis; School of Oriental and African Studies, University of London, 1996), pp.142-60.
[114] Although little reference is made in this essay to one of the most important – the Portuguese Empire – and none to the equally notable Dutch Empire, or indeed to south-east Asia including the Philippines, or to the Pacific and Australasia, most were the scene of epidemic catastrophe and inoculation attempts before the close of the eighteenth century and the discovery of vaccination.
[115] Inoculation has been seen as a jewel in the crown of the Enlightenment, and although this essay does not include specific evaluation of the topic, honourable mention must be made here of Charles-Marie de La Condamine (1701-1774) − traveller, geographer, mathematician and historian – some part at least of whose persistent advocacy of the operation and his unrelenting attention to its history − was usually available in print as recorded in the bibliography below.
[116] Miller, The Adoption of Inoculation, pp.190-1, cites the activities of Jean Delacoste in the early 1720s.
[117] Sköld, P., The history of smallpox and its prevention in Sweden (Umeå, 2002). This account covers the nineteenth and twentieth centuries as well as the eighteenth but on p.78 it confirms the pre-Suttonian visit of Schultz to England in 1754 and the interest of the Medical Board from 1756, vindicating Klebs’s account of early Swedish concern with public health. It also contains (p.77) a demonstration of how rural parishes directly connected to roads were the most severely affected by smallpox mortality.
[118] A. Eriksen, ‘Cure or Protection? The meaning of smallpox inoculation, ca 1750-1775’, Medical History, 57, 4 (2013), pp.516-536.
[119] Medicalisation. A term used to describe increasing exposure of populations to medical oversight and treatment from the eighteenth century onwards. F. Loetz, ‘“Medikalisierung” in Frankreich, Grossbritannien und Deutschland, 1750-1850’, in W. Eckhart and R. Jutte (eds), Das europäische Gesundheitssystem. Gemeinsamkeiten und Unterschiede in historische Perspektive (Stuttgart, 1994).
[120] Ibid. pp.123-4. The French overview summarised – that of P. Goubert.
[121] Ibid. pp.124-5. The German overview – that of U. Frevert.
[122] Ibid. pp.125-6. The English overview – R. Porter.
[123] A. Macfarlane, Thomas Malthus and the making of the modern world (Amazon CreateSpace, [2014]), p.5. Discussion of why mortality dropped sharply in England in the eighteenth century for reasons which were largely (with the possible exception of smallpox inoculation) unrelated to medical improvements.
[124] Klebs, ‘The historic evolution of variolation’, p.83.
[125] Miller, The Adoption of Inoculation, p. 20.
[126] Darmon, Emch-Dériaz, Seth.
[127] Lobo, May, Razzel, Rusnock.
[128] Brunton.
[129] Dryvik, Eriksen, Sköld.
[130] Sonntag.
[131] Maehle.
[132] Bartlett, Renner.
[133] Brimnes
[134] Inoculation required legislation to ban it in England as late as 1840.
[135] Opinion is divided as to whether the Suttons’ business continued to prosper in England towards the end of the century. Smith concludes that it failed but Razzell takes the opposite view. See Smith, The speckled monster, pp.85-7, and Razzell, ‘The decline of adult smallpox in eighteenth-century London: a commentary’, p.1322.
[136] J. William Frost (ed.), The Records and Recollections of James Jenkins Respecting himself, and others from 1761 to 1821, being a period of sixty years − with Additions tending to illustrate the whole, Texts and Studies in Religion, vol.18, (New York and Toronto, c.1984). Jenkins claimed a sighting of the eighty-nine-year-old in Hertford Market and assumed that as an opponent of Lettsom and of Jenner and vaccination too, Dimsdale resembled ‘the Turk who bears no rival near the throne’− an allusion to Pope’s satire on the character of Joseph Addison.
[137] Jenner, An Inquiry into the Causes and Effects of the Variolae Vaccinae; Beale, Echoes of Ingen Housz, pp.496-506.
[138] The Rector of Little Berkhamsted Richard Levett’s afterthought noted in a Parish Register. Hertfordshire Archives and Local Studies DP/20/1/2.
© Robert Dimsdale, 2017